
- Reference Number: HEY107/2023
- Departments: Maternity Services
- Last Updated: 30 June 2023
Introduction
This leaflet has been produced to give you general information about the procedure of induction of labour. Most of your questions should be answered by this leaflet. It is not intended to replace the discussion between you and your midwife or doctor but may act as a starting point for discussion. If after reading it you have any concerns or require further explanation, please discuss this with the midwife or doctor.
What is induction of labour?
In order for a baby to be born the cervix (the neck or opening to the womb) has to shorten, soften and open and there must be contractions. Your womb has a powerful muscular wall that tightens and then relaxes; these contractions gradually open your cervix. In most pregnancies this starts naturally between 37 – 42 weeks and is called ‘spontaneous labour’. Induction of labour is a process used to encourage labour to start artificially.
When might I be offered induction of labour?
There are three main reasons why induction of labour (IOL) is offered:
- Prolonged pregnancy – pregnancy that continues after 41 weeks. After 41 weeks there is a slight increase in the risk of your baby developing health problems. We therefore recommend Induction of labour between 41 and 42 weeks.
- Pre-labour rupture of membranes – (the waters around the baby breaking) if spontaneous labour does not happen approximately 24 hours after the waters break there is a small risk of infection to the mother and/or the baby.
- Medical reasons – If it is felt that your health or your baby’s health is at increased risk if the pregnancy continues.
Can I choose not to be induced?
After considering all the facts around IOL, if you decide you do not want to be induced, you should tell your midwife. You can be offered an appointment to attend hospital so we can check that you and your baby are well and there will be an opportunity to discuss with a midwife or doctor your decision not to be induced.
How often you come to the hospital for checks depends on your situation. The midwife or doctor will discuss this with you.
Membrane Sweep (stretch and sweep)
Once you have reached your due date, you will be offered a membrane sweep at around 40 weeks, followed by another at 41 weeks. This procedure has been shown to increase the chances of labour starting naturally within 48 hours of the procedure and can reduce the need for other methods of induction of labour.
You will also be offered a membrane sweep if induction of labour is being done for medical reasons. The timing will be advised by the doctor responsible for your care.
A stretch and sweep is a vaginal examination that can be carried out at home or at an Antenatal Clinic. The procedure involves the doctor or midwife putting two fingers inside your cervix and making a circular sweeping movement to separate the membranes from the cervix. This increases the production of hormones called prostaglandins which can encourage labour to start.
There may be some discomfort or bleeding but it will not cause any harm to you or your baby. It will not increase the chance of you or your baby getting an infection.
Where will labour be induced?
The majority of women will be managed in an outpatient setting. All women come to an Induction of Labour Clinic to have the procedure started.
Most women will be able to go home afterwards, but sometimes you will have to stay in hospital because of medical reasons or the method of induction being used. Please pack a birth bag and either bring it with you or have it available in your car. If your cervix is favourable to have the waters around your baby broken or the waters have already broken (pre-labour rupture of membranes) you will be induced on the Labour Ward. Please be aware that breaking the water around the baby can only be done on Labour Ward. Admission to the Labour Ward will be managed according to individual needs and this may happen straight away or more likely you will be asked to wait at home until you are called to attend Labour Ward.
An outpatient induction of labour:
- Reduces the amount of time you will need to stay in hospital before your labour begins.
- Allows you to stay at home which evidence has shown helps labour to progress as you are in a familiar place.
- Makes the process of induction as close as possible to going into labour naturally
Your midwife or doctor will assess if you are suitable for outpatient induction of labour and discuss this with you.
At very busy times, the start of the induction process may be delayed. Very rarely it may be delayed for over 48 hours. If you are at home, you may be advised to come in to the Induction Clinic to have an antenatal review and to monitor your baby with a cardiotocograph (CTG) machine. You will be able to go home afterwards if there are no concerns about you or your baby.
What will happen?
When you come to clinic the midwife will introduce themselves and discuss everything with you to make sure you understand the procedure. Please feel free to ask any questions or voice any concerns or anxieties. We are here to help at all times.
While you are in clinic or on the Labour Ward you can have up to two birth partners with you all the time. If you are admitted to the Antenatal Ward just one birth partner can be with you all the time.
When you arrive, the midwife will do a full antenatal check on your baby and you. Your baby’s heartbeat will be monitored using a cardiotograph (CTG) machine that gives a paper recording of the heartbeat.
You will have a vaginal examination to determine how favourable your cervix is to break your waters (Artificial Rupture of Membranes). If your cervix is not favourable then one of the methods below will be used.
Methods used to prepare the cervix
These are used to soften and open the cervix in order to be able to ‘break the waters’ around the baby. They may sometimes cause contractions to start as well.
You may need just one or all of these methods.
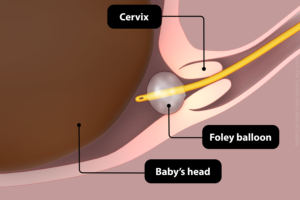
Cervical Ripening Balloon Catheter
The balloon catheter is the only method used for outpatient induction of labour. This is because it has minimal side effects and does not need you to be monitored as closely as when using a medical method.
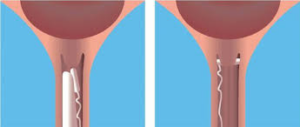
The procedure involves a catheter (a soft silicone tube) being inserted into your cervix. It has a balloon near the tip and when it is in place the balloon is filled with a sterile saline (salt water) fluid. The catheter stays in place for 24 hours, with the balloon putting gentle pressure on your cervix. The pressure should soften and open your cervix enough to be able to break the waters around your baby or it may start labour. It is important to realise that this does not happen for everyone and you may need to progress to other methods.
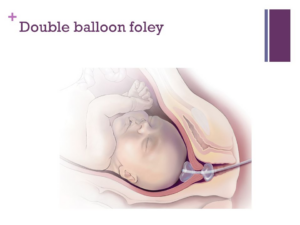
Sometimes a double balloon is used especially if your cervix is very long or hard. It works the same as a single balloon
The balloon catheter may fall out by itself or will be removed by a midwife the following day.
Going home after cervical ripening balloon catheter
During the time you are at home, you can do things as you would normally, for example, showering, bathing or walking. However, please avoid intercourse. After going to the toilet please wash your hands, make sure the catheter is clean and change underwear regularly.
If you have any of the following:
- Bleeding
- Contractions
- Concerns about the baby’s movements
Or
- You feel unwell
- The waters around the baby break
- The balloon falls out
You are advised to call Maple Ward on (01482) 607779. A midwife will talk with you and advise you what you need to do.
Prostaglandin
Prostaglandin is a hormone that is naturally produced by the body. It is involved in starting labour. We use two methods to deliver an artificial version of prostaglandin.
- A pessary known as ‘Propess’® is inserted into the vagina and place behind the cervix. It has tape attached so it can be removed easily. It releases the hormone slowly over 24 hours but will be removed earlier if labour starts or there are any concerns about you or your baby’s health.
- A tablet called ‘Prostin’® is inserted into the vagina and next to the cervix. You will be re-examined six hours after the first tablet; if the cervix is still not ready for the waters to be broken or you have not started in labour then a second Prostin® tablet will be inserted into the vagina.
You will have to stay in hospital if these methods are used, as your baby will need to be monitored every eight hours. Between monitoring, you will be encouraged to walk about or use the ‘birthing balls’, as being active can help to encourage labour to start.
It is important to be aware that the process of softening and opening the cervix can take up to three days if you are over 41 weeks and up to five days if we are inducing you earlier than 41 weeks. It is also important to know that it may fail completely.
When the cervix is favourable to have the waters around the baby broken, known as an Artificial Rupture of Membranes (ARM), you may be able to go home and, unless you go into labour spontaneously, you will be contacted by the Labour Ward with a time for admission.
This may also take up to five days. The consultant in charge of the Labour Ward will make a decision about when to admit you to the Labour Ward based on medical needs and at all times keeping in mind the safety of your baby and you. If you are being induced as an outpatient, this will NOT affect the decision about when you will be admitted to the Labour Ward.
While you are waiting you may be offered extra assessment and monitoring of the baby. How often this happens will depend on the reason why you are being induced.
Previous Caesarean Section
If you have had a previous Caesarean Section, you will only be offered the balloon catheter as a means of inducing labour. You may be offered another balloon catheter if the first one is not successful. You will not be offered prostaglandin as it increases the chance of the scar separating or tearing.
What happens next
When the cervix is favourable to have the waters around the baby broken, known as an Artificial Rupture of Membranes (ARM), you may be able to go home and wait to be contacted by the Labour Ward with a time for admission.
THIS CAN TAKE UP TO FIVE DAYS. The consultant in charge of the Labour Ward will make a decision about when to admit you to the Labour Ward based on medical needs and at all times keeping in mind the safety of your baby and you. If you are being induced because you are Post-dates (over 41 weeks) you will be a priority to go to Labour ward.
If you are being induced as an outpatient, this will NOT affect the decision about when you will be admitted to the Labour Ward.
During this ‘waiting time’ you will be offered appointments in the Induction Clinic so we can monitor your baby and yourself and give membrane sweeps if you want. How often this happens will depend on the reason why you are being induced.
If your waters break by themselves then you may be able to wait to see if you go into labour. If you do not, then labour will be induced with the hormone drip approximately 24 hours following the waters’ breaking.
If you go into labour by yourself, you are no longer on a ‘waiting list’ but will be admitted to the Labour Ward or Midwifery -Led Unit when labour is established.
If the process has failed you will be offered a planned Caesarean Section. Your Consultant and the ward staff will arrange all this for you.
What happens on the Labour Ward
Artificial rupture of the membranes (ARM)
When the cervix is soft, open to around two to three centimeters and the baby’s head has gone down into your pelvis, it should be possible to ‘break the waters’ around the baby.
This procedure is carried out by using a small plastic hook which releases the water and allows the pressure of the baby’s head to press on the cervix and stimulate contractions. It will not harm you or your baby. The procedure may be uncomfortable but it should not be painful.
You may be given some time to see if contractions start or we may use an artificial hormone called Syntocinon® straight away.
Oxytocin (Syntocinon®)
This is an artificial form of the hormone that causes your uterus (womb) to start having contractions.
It is given through a tiny tube into a vein in your arm (drip). It can only be given when your waters have broken.
The drip is increased very slowly until your uterus is contracting regularly and strongly. Women respond differently to how well the drip works on contractions and it also depends upon how ready your body is for the labour process.
During labour, your baby’s heart rate will be monitored continuously by a cardiotocography (CTG). Your ability to walk around will be limited by the drip and monitor, although you may choose to stand up or sit on a chair or birthing ball.
The Syntocinon® drip is the main form of induction when your waters have broken naturally and you do not go into labour.
We will endeavour to induce labour by 24 hours following rupture of membranes, however this may not always be possible. Please be assured that all decisions are made with regards to the safety of your baby and you. If your induction is delayed, you will be asked to come to the hospital Antenatal Clinic/Day Unit so that your baby and you can be assessed and monitored.
Can there be any complications or risks?
Cervical Ripening Balloon Catheter
The procedure can be uncomfortable but it should not be very painful. You may get strong period cramps after the balloon is inserted, usually these die off after a few hours. It is suggested that you have some pain relief ready at home for this. Paracetamol or Co-codamol is fine to take in pregnancy. We may give you some strong Co-codamol to take home with you if you need it.
There is a very small risk of infection. If an infection is suspected, your baby will need to be delivered by the quickest possible method. So, it is VERY important to let us know if you think your waters have broken while the balloon is still in.
Prostaglandin (Prostin®)
Inserting the prostaglandin pessary can be uncomfortable. Prostaglandin can cause dryness and soreness in and around the vagina. It can also cause strong contractions, which can be painful; having these contractions does not always mean you are in labour. Your midwife will discuss ways to help you manage this.
On rare occasions prostaglandins can cause the uterus to contract too frequently and this may affect the pattern of your baby’s heartbeat. This is usually treated by giving a drug that helps the uterus to relax. Sometimes the uterus continues to contract too frequently, which may mean an emergency caesarean section is necessary.
Oxytocin (Syntocinon®)
As with prostaglandin, the main risk is that the uterus can contract too strongly/frequently and affect the baby’s heartbeat. Reducing the rate of the Oxytocin can have an immediate effect on easing the contractions, which will improve the baby’s heartbeat. If the baby’s heartbeat does not recover, the senior doctors will decide what is required. This may mean an emergency caesarean section is necessary.
What happens if induction of labour fails?
In a small number of cases induction of labour is not successful following repeated attempts. Your management will then be discussed with your consultant obstetrician and a plan for birth put into place. It may be that a caesarean section is recommended.
How do I prepare for induction of labour?
Please read this information leaflet and share the information it contains with your partner and family (if you wish) so that they can be of help and support. There may be information they need to know, especially if they are supporting you as the birth partner/s.
We recommend making family, especially children and those caring for them ,and friends aware that the procedure can take a long time (in some cases up to 10 days) before the baby is born.
You may want to nominate one person to give the rest of the family updates on how things are progressing.
You can bring one birth partner to Induction Clinic with you.
It is advisable to wear loose clothing when coming to the Induction Clinic as it will be more comfortable when you are being examined.
If you are admitted to the Antenatal Ward (Maple Ward), wear clothes you are comfortable in. It is not necessary to wear night clothes in the day as we actively encourage you to be mobile, depending on any medical condition you may have.
You may bring a book, magazines and games to keep you occupied due to the length of time the procedure may take.
There are television and telephone consoles by each bed and there is a secure mobile phone charging station on the ward. MOBILE PHONES SHOULD NOT BE CHARGED BY THE BED.
Please ask the ward staff for current visiting times.
Should you require further advice on the issues contained in this leaflet, please do not hesitate to contact Maple Ward tel: 01482 607438
